
“The cartilage doc” – preserving joints instead of replacing them
Osteoarthritis
My basic treatment approach for osteoarthritis: preserve joints instead of replacing them
Osteoarthritis is the most widespread joint disease in the world. Sufferers feel pain, especially in the morning and during exertion. Sometimes the joints even make themselves felt at night. In X-rays and MRI scans, the protective cartilage becomes thinner or is completely missing. This objective “finding” does not necessarily correlate with the patient’s “complaints“. Orthopaedic surgeons should not treat images, but the complaints of their patients. The patient suffers above all when their osteoarthritis “activates“. This is the case when the joint becomes inflamed. Due to the inflammation, anti-inflammatory drugs such as cortisone, ibuprofen, diclofenac and similar medications also help in the short term. If you want to do something for your joint health in the long term, you need to treat the joint metabolism and address other risk factors in addition to acute inflammation.
Our understanding of osteoarthritis is changing. Osteoarthritis is a chronic disease of the joint and not just purely mechanical wear and tear. This also changes the therapeutic options. A worn-out car tire cannot regenerate, but cartilage damage can. In the case of pronounced mechanical changes that impair the mobility of a joint due to bony growths (lat.: osteophytes) or free joint bodies, surgical treatment makes sense for those affected. Germany is one of the world’s leading countries in the field of joint replacement surgery, i.e. arthroplasty. However, it is very often possible to preserve a joint with cartilage damage. I will explain these options below.

Get to know the guide for patients with joint wear and tear!
What therapies are available?
There are numerous therapy options for the treatment of osteoarthritis. We discuss which measures are sensible and promising as part of a personalized osteoarthritis therapy together at the start of treatment.
In my guide “The osteoarthritis consultation” I explain a holistic concept for your joint health. Those affected have many opportunities to influence the course of their osteoarthritis. Exercise, diet and reducing damaging behavior are just a few examples. On this page, I would like to explain how I can support you medically with joint-preserving therapy.
There are various regenerative therapy methods. We also speak of orthobiological therapies. We use them to exploit the regenerative potential of our body. The aim is to inhibit inflammation, improve joint metabolism and, as a result, reduce pain and improve function. These are primarily hyaluronic acid, the body’s own plasma and regenerative cells from fatty tissue. These are particularly effective due to the stem cells they contain.
What factors influence the choice of therapy and its success?
There are a number of ways to treat osteoarthritis conservatively. The size, depth and localization of the cartilage damage are decisive factors in the treatment decision. These are determined with the help of radiological imaging.
The individual factors of the patient are very important for complaints. These include body weight, training condition, diet, occupational and sporting stress on the joint and the patient’s demands.

Isolated deep damage to the cartilage with an extension of up to 2 x 2 centimetres can often be “repaired” surgically. I use various surgical procedures for this, mostly microfracturing in combination with a matrix / membrane and autologous, one-sided cartilage transplantation (AutoCart method). Larger damage and cartilage injuries in several joint sections are often better suited to injection treatment with SVF/ACP.
Larger damage with a shallow depth is usually treated with injections. More on this in the next point -> Depth of the cartilage defect.


In addition to the size of the cartilage damage on the surface, the depth is also decisive. Damage ranges from superficial damage (grade 1) to complete cartilage loss (grade 4) and exposed bone.
Frequently used classifications of cartilage damage use four degrees of severity (e.g. the classification according to Outerbridge or that of the International Cartilage Research Society).
In grades 1 and 2, cartilage therapy is almost exclusively conservative. Conservative and surgical treatments are possible for grade 3 and 4.

Cartilage damage to the knee
Several joints are often affected by osteoarthritis at the same time. Surgical therapies can often only be carried out on one joint at a time, as postoperative relief or partial weight-bearing is required for several weeks. Orthobiological / regenerative therapy can be carried out on several joints at the same time. I treat up to four joints at the same time, for example both knee and hip joints.
Joint-preserving therapy also means that “no bridges are burned”. Surgery is still possible if the treatment results are inadequate.
Our “musculoskeletal” system requires regular training. A sedentary lifestyle combined with increasing age leads to deficits in the areas of mobility, strength and neuromuscular movement control. This can promote osteoarthritis and exacerbate its symptoms.
Conversely, targeted exercise can alleviate the symptoms of osteoarthritis. Exercise is one of the most effective forms of medication. It must also be used just as carefully as medication.
My team of three sports scientists carry out a movement analysis and then guide you through targeted functional training. We also use innovative forms of training that are particularly successful for osteoarthritis, such as Kaatsu and EMS training.
You can also find tips on the subject of training in my book “Return to Sport.

Our body is constantly renewing itself. To do this, it needs nutrients and building materials. An adequate supply of nutrients therefore protects our muscles, bones and cartilage. Our diet can also promote or reduce inflammation. There are numerous books on the subject of osteoarthritis and nutrition.
I also cover the essential information in my book “TheOsteoarthritis Consultation“. An anti-inflammatory diet can noticeably alleviate the symptoms of osteoarthritis and reduce the intake of painkillers. We can check whether we are sufficiently supplied with vitamins, micronutrients and omega-3 fatty acids, for example, with a blood count.
If there are deficiencies, these can be compensated for through nutrition or dietary supplements.
Our diet affects our body weight – for better or for worse. Every extra kilo has to be supported by our joints. Body weight is therefore a decisive factor for the success of therapy.
With a body composition analysis on the InBody scale we determine the current state of your body composition. In addition to adjusting your diet, we can of course also change your body weight through targeted training. With currently three sports scientists in my team, we also offer training advice.
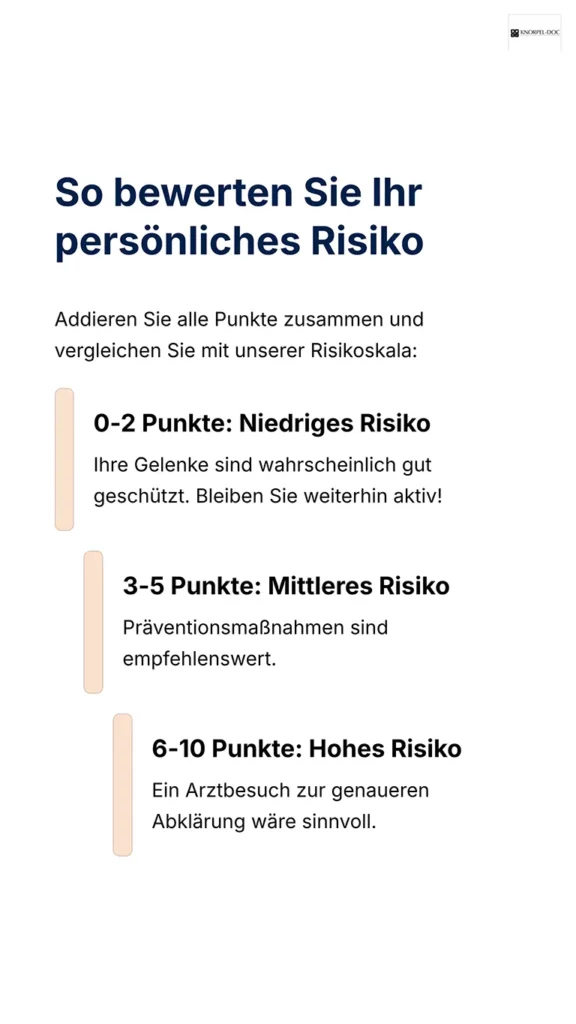
Osteoarthritis self-test
As an expert in osteoarthritis therapy, I offer you an image-based osteoarthritis self-test to help you assess your personal risk in just a few steps.
Look at the pictures and add up your points at the end.
What you get out of it: I will show you which signs indicate a possible joint strain. Important: This self-test does not replace a medical diagnosis. If you have severe or persistent symptoms, please make an appointment.



Better results through scientific monitoring of your therapy
The possibilities for treating osteoarthritis are constantly evolving. In order to check the quality of my care and the effectiveness of innovative therapies, I have been scientifically evaluating treatments for many years. To this end, I cooperate with the University of Bielefeld, Charité and the International Cartilage Research Society (ICRS).
I therefore ask my patients to answer a few web-based questions during treatment with Sinogel (hyaluronic acid), stem cells (SVF/ACP) and arthrosamide. The survey is carried out at the time of treatment, after 3, 6 and 9 months and then once a year. Various orthopaedic scores are determined, which cover the areas of pain perception, joint mobility and resilience as well as quality of life.
Patients can register under this link before undergoing orthobiologic treatment of the knee joint.
What treatment options do I have for joint-preserving osteoarthritis therapy?
My aim is to preserve joints rather than replace them. In the case of cartilage damage that cannot be repaired surgically, I primarily use orthobiological substances.
Hyaluronic acid improves the cartilage’s ability to bind water and thus supports its buffering effect. To put it metaphorically: a sponge with numerous holes can only absorb water where sponge tissue is still present. This is why hyaluronic acid is particularly effective for mild to moderate cartilage damage (grade 1-2) – newer preparations such as Sinogel still show good effects even at grade 3.
Hyaluronic acid also has an anti-inflammatory effect and reduces friction in the joint. The available preparations differ in their viscosity, dwell time in the joint and their additives – some are monopreparations (single injection), others are administered 3-5 times. The effect sets in individually within days to weeks.
Combination therapy with ACP/PRP:
Combined therapy with ACP (autologous conditioned plasma) is particularly effective. Studies show that this combination significantly increases the effectiveness compared to monotherapies – hyaluronic acid optimizes the gliding ability, while ACP promotes the body’s own regeneration and inhibition of inflammation. This synergistic effect makes the combination particularly attractive for moderate cartilage damage.
Costs:
In most cases, the therapy costs are covered by private health insurance companies. Patients with statutory health insurance can be treated as self-payers.
ACP – Autologous Conditioned Plasma
Platelet-rich plasma (PRP) has been used successfully in orthopaedics for over 10 years to treat osteoarthritis. Since 2016, I have performed over 3,000 therapies (as of April 2024) with ACP.
Therapeutic mechanism
Compared to hyaluronic acid, plasma treatment activates the body’s own regeneration and has an increased anti-inflammatory effect. During treatment, the patient receives only their own plasma without any additives, which maximizes biocompatibility and effectiveness.
Therapy spectrum: from standard ACP to Angel PRP
My therapy spectrum now includes several PRP technologies that differ in terms of cell concentration and therefore therapeutic potency:
Standard ACP is suitable for mild to moderate cartilage damage (grade 1-3) and is usually administered 3-5 times per joint. The effect sets in individually within a few days to weeks.
ACP max offers a higher concentration of platelets and bioactive substances, which enables a more intensive regenerative effect – ideal for patients with more severe damage or when faster results are required.
Angel PRP uses an extremely advanced centrifugation technology that achieves an exceptionally high cell count and therefore maximum therapeutic concentration. This technology is used by less than 10 practitioners across Germany. Angel PRP allows for more precise and potentially more effective treatment, especially for more complex degeneration.
The importance of high cell counts
The therapeutic efficacy of PRP is directly dependent on the quality and concentration of platelets and growth factors.
A high cell count is crucial for..:
Not all PRP systems achieve the same high concentrations – this is a major difference between standard procedures and state-of-the-art systems such as Angel.
Quality control through cell count measurement
To ensure the highest possible treatment quality, we carry out quality control of the cell counts. Before each injection, the exact cell counts and the concentration of biologically active substances are measured and documented.
This enables us to:
Indications and repetition
A good indication for ACP is mild to moderate cartilage damage (grade 1-3). In osteoarthritis, ACP treatment should be repeated at regular intervals, usually once a year, in order to maintain and enhance the therapeutic effect.
Scientific evidence
The study situation for the use of ACP in osteoarthritis is now very good. National and international specialist societies recommend the use of blood plasma for osteoarthritis (AGA, ESSKA).
Further areas of application for PRP
The therapeutic spectrum of PRP extends beyond the treatment of osteoarthritis:
Costs and cost coverage
In most cases, the therapy costs are covered by private health insurance companies. Patients with statutory health insurance can pay for these treatments themselves.
Patient behavior before therapy plays a major role in ACP therapy!

For advanced cartilage damage, I use the high regenerative potential of the body’s own stem cells from fatty tissue. MFAT contains a large number of regenerative cells and so-called “medical signaling cells” that control regeneration in the joint.
A good indication is high-grade cartilage damage (grade 3-4). Since 2017, I have treated over 1,700 patients with this method – making it the most therapies I have performed in the German-speaking world.
Treatment procedure
In an outpatient treatment under local anesthesia, fatty tissue is removed from the abdomen or thigh and processed directly – either with Lipogem or MFAT) using the procedure from JOINTEC Labs. The stem cells are then injected into the affected joint. The entire treatment takes about two hours.
Scientific evidence
The study situation is very good. Quality-tested studies and meta-analyses prove the effective effect of MFAT in high-grade osteoarthritis with a low risk of side effects. National and international professional societies recognize the evidence.
Effect
The effect sets in on average between 2 weeks and 2 months. A supplementary ACP booster per year reinforces and prolongs the effect.
Scientific monitoring
I evaluate treatments scientifically: Patients answer standardized questions at the time of therapy, after 3, 6 and 9 months and annually. This enables continuous optimization of the therapy.
Costs
Costs are often covered by private health insurance companies. Those with statutory health insurance can be treated as self-payers. The costs start at €1,500 for the first joint plus materials and imaging if required. Further joints start at an additional €200.
In the case of advanced cartilage damage, I rely on the high regenerative potential of the body’s own stem cells or, more precisely, on the “stromal vascular fraction” (SVF). This is a component of our fat cells. It is rich in regenerative cells, including connective tissue stem cells. They are also referred to as “medical signaling cells“, as they control regeneration in the joint like a conductor.
High-grade cartilage damage (grade 3-4) is a good indication for the therapy. As of April 2024, I have treated over 800 patients in this way since 2017. This means I have carried out the most therapies in the German-speaking world.
In an outpatient treatment, fat cells are harvested from the subcutaneous fatty tissue on the abdomen or thigh under local anesthesia and processed directly. The joint to be treated is also anesthetized locally and then injected. The treatment takes about two hours, including preparation and follow-up. As a rule, only one treatment is carried out.
On average, the treatment takes between 2 weeks and 2 months to take effect. The effect of the therapy can be enhanced by additional injections of ACP, collagen and hyaluronic acid. I refer to this as a “booster“. This should be carried out on average once a year or earlier depending on the complaint.
The study situation for this still young therapy method proves the good effect even with higher-grade osteoarthritis with a low risk of undesirable side effects.
Other areas of application are
The therapy costs are often covered by private health insurance companies. Patients with statutory health insurance can be treated as self-payers. Treatment costs start at €1,500 for one joint. For several joints, the additional costs per joint are lower.


Collagen is a component of the cartilage matrix, i.e. the connective tissue that surrounds the cartilage cells. There are different types of collagen that occur in various tissues, including cartilage tissue. Collagen type II in particular is found in cartilage and plays an important role in its structure and elasticity.
An injection of collagen for osteoarthritis can reduce pain and improve the gliding behavior of the joint. I use collagen for moderate to severe cartilage damage (grade 2-4) in addition to ACP / SVF. Three injections are given every 40 days, on days 1, 14 and 40. Some patients also benefit from a regular supply of hydrolyzed collagen in the form of a dietary supplement.
In most cases, the therapy costs are covered by private health insurance companies. Patients with statutory health insurance can be treated as self-payers.
The one-off injection of arthrosamide is a relatively new treatment method for osteoarthritis on the German market. It is an injectable hydrogel that is permanently deposited in the synovial membrane (“synovia”) and binds water there. This reduces the painful inflammation of the synovial membrane (“synovialitis”) in activated osteoarthritis.
This substance is currently only approved for osteoarthritis of the knee joint. According to the manufacturer, the patient receives a “single-shot antibiotic” immediately before the therapy. This involves two antibiotic tablets for prophylaxis against infections. The effect of the injection sets in on average within the first two to four weeks. In the first few days after treatment, unusually intense physical exertion should be avoided. The usual medication and, if necessary, painkillers can be taken unchanged.
The injection is usually only given once, as the effect often lasts for several years if there is a good response.
The treatment of other joints can only be carried out as “off-label” therapy. I have had good experiences in the shoulder area, which I have also published as a case report. Treatment with Arthrosamide can generally be combined well with the other methods.
In most cases, the therapy costs are covered by private health insurance companies. Patients with statutory health insurance can be treated as self-payers.
Bone marrow edema is a significant factor in the progression of osteoarthritis. They occur frequently in patients with activated osteoarthritis and are associated with faster disease progression and poorer prognoses. The subchondral bone is overloaded by the edema, resulting in local circulatory disorders and microfractures – a vicious circle that can lead to bone necrosis and accelerated joint degeneration if left untreated.
Outpatient IOBP – a unique selling point in Germany
While Intraosseous BioPlasty (IOBP) has been performed in the USA for decades with excellent results, I have been performing this innovative treatment as a pioneer in Germany on an outpatient basis since 2024 – under local sedation and CT guidance. This is a unique selling point in Germany.
The treatment can either be performed on an outpatient basis or combined with arthroscopy and MFAT therapy in the operating theater. In the outpatient variant, a core decompression and direct access to the bone marrow edema is created under sedation and CT control. I then inject highly concentrated ANGEL PRP – obtained directly from the blood or bone marrow – to stimulate physiological bone regeneration.
Scientific evidence
The study situation is excellent. Decades of American experience show significant pain reduction after just one week (VAS from 8.3 to 1.5) and sustained functional improvements over 12 months. The IOBP technique shows a 93% joint preservation rate at 1-year follow-up, with 75% complete edema healing in the MRI control. The procedure is safe, with a low complication rate.
Follow-up treatment
After treatment, the patient should rest for 2 weeks with thrombosis prophylaxis. However, most patients experience a significant reduction in symptoms within the first few days.
Scientific monitoring
As with the other orthobiological therapies, I also evaluate the IOBP treatments scientifically – with standardized questions on pain, function and quality of life at regular intervals.
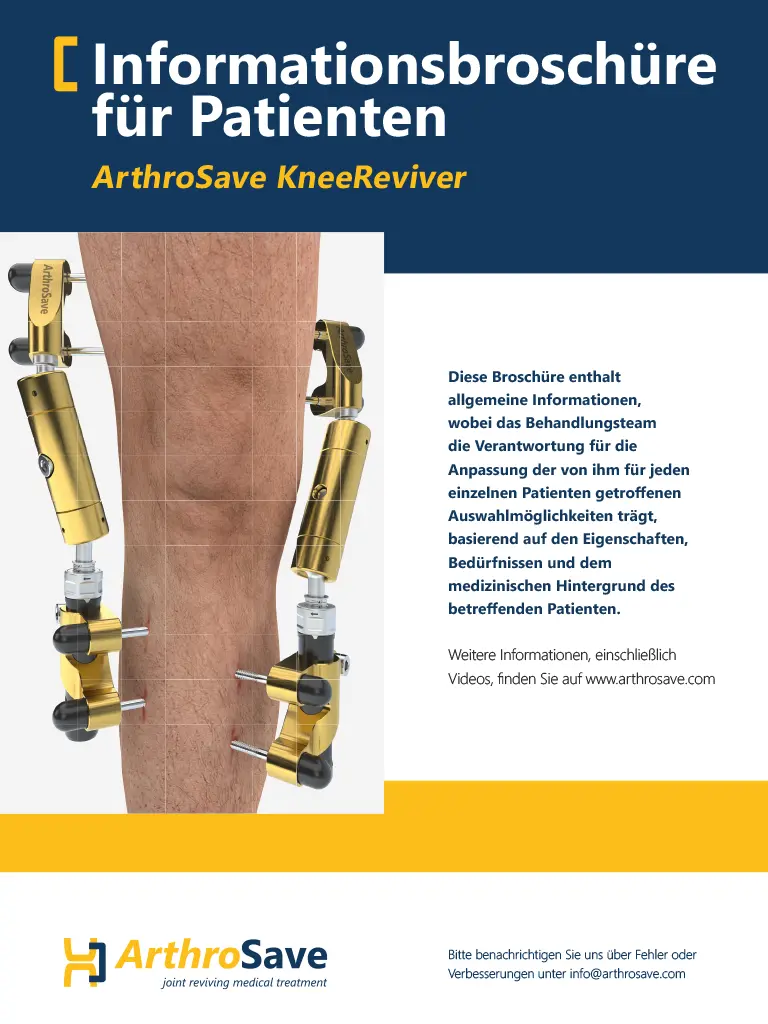
Knee distraction (knee joint distraction) is a joint-preserving procedure for advanced osteoarthritis of the knee that uses an external fixator to enlarge the joint space for a few weeks in order to reduce pain, improve function and achieve structural effects (especially an increase in cartilage and joint space). The method is primarily aimed at “too young” endoprosthesis candidates (<65 years) in order to postpone joint replacement for years.
Principle and technique
In the classic procedure, transosseous pins are inserted into the femur and tibia and connected via an external frame (e.g. KneeReviver); the joint is then distracted by a total of around 4-5 mm for around six weeks. During the distraction phase, full or partial weight-bearing with walking aids is usually permitted, but the joint remains pressure-relieved, which is intended to trigger mechanobiological regeneration processes in the cartilage and subchondral bone.
Indications and patient profile
The typical indication is pronounced, usually medial gonarthrosis in patients with severe pain who have exhausted conservative measures (including injections) and who, according to guidelines, would actually be candidates for a prosthesis but are still relatively young. Exclusion criteria include severe axial deformities, unstable ligaments, pronounced inflammation, infection, poor bone status or relevant comorbidities that make external fixation risky.
Results and evidence
Long-term data (mainly Utrecht group, >10-year follow-up) show significant pain reduction, functional improvement (knee scores) and radiologically measurable joint space and cartilage increase over several years in many patients. On average, the need for primary TKA can be postponed by around 5-10 years, with some patients still managing without a prosthesis after a decade.
Risks and limitations
The main problems are pin-track infections, risk of thrombosis/embolism, risk of falling, joint stiffness and the psychosocial burden of the fixator for weeks. In addition, the procedure is logistically complex, requires experienced centers and close physiotherapeutic supervision; robust randomized comparisons with arthroplasty or structured conservative programs are still limited.

Illustration ArthroSave KneeReviver
Various procedures are available for the surgical treatment of cartilage damage. Cartilage smoothing is intended to slow down the progression of the damage, but does not repair it. Chronic painful irritation of the bone – bone marrow edema – can also be drilled and treated orthobiologically with ACP.
Bone marrow stimulation procedures use the healing potential of the bone to form replacement cartilage tissue. This procedure is more successful if a matrix, a membrane that acts like a “plaster”, is also used.
There are cell-based procedures in which cartilage is cultivated after a sample is taken and used in a second operation. Alternatively, cartilage tissue can also be obtained from unloaded joint areas in a single operation, processed and applied directly to the damaged area. I prefer to use this procedure. The name of the operation – AutoCart – sums up the concept well. The patient’s own “cartilage” is used.
A bow leg or knock-knee can be corrected with a corrective osteotomy, particularly at the knee joint. This involves surgically correcting the leg axis.
Relieving orthoses, which I often prescribe in addition to conservative or surgical therapy, are also based on this concept of relief through weight transfer.
The choice of the right procedure depends on the size and localization of the cartilage damage, concomitant diseases and the age of the patient.
In most cases, the therapy costs are covered by statutory and private health insurance companies. As I run a private practice, I can treat patients with statutory health insurance as self-payers if they wish.

How does treatment work?
The first step is a detailed consultation, a physical examination and an assessment of the radiological imaging. Our own radiologists can produce MRI, CT, DVT or X-ray images at short notice. Appointments can be made in combination with imaging.
Existing images can be uploaded to our practice system in advance via the following link.
If you have to travel a long way, an initial assessment can also be carried out by telephone before SVF / ACP / MFAT (stem cell) therapy, provided that recent images from the last 12 months are uploaded to us.
The severity of the cartilage defect, the joint mobility and the level of pain and your requirements are decisive criteria for the treatment decision. At the end of the consultation, we will decide together how to proceed if you wish to be treated by me.

Cartilage transplantation for osteoarthritis of the knee joint with AutoCart
The treatment is usually performed on an outpatient basis. Anesthesia for SVF / ACP / MFAT is administered locally on the abdomen and the joint. The other injections are preceded by cold therapy of the joint (Cryofos).
This means that you can arrive and depart yourself. For a very long journey of several hours, I recommend an overnight stay on site, at least for SVF / ACP / MFAT therapy.

Treatment with cryotherapy (Cryofos)
I usually carry out controlled injections using ultrasound or CT. This ensures that the joint is hit safely. Scientific studies show that injections into joints without imaging often do not achieve their goal. Patients can put weight on their joints immediately after treatment. In some cases, the treated joints may be temporarily painful and feel swollen in the first few days. These symptoms usually subside within the first two weeks. Very physically demanding or unaccustomed strain should be avoided during this time.
In the case of orthobiological treatment with SVF, MFAT, Lipogem, Arthrosamide and IOBP, I recommend resting for the first two weeks after treatment

Injection controlled by ultrasound
Here you can find more information on osteoarthritis treatment with the body’s own stem cells:
Do you have any questions or would you like to make an appointment? With pleasure!
Appointments can be made by telephone or e-mail.
If no current images are available, imaging can be combined with the orthopaedic presentation. Existing images and findings can be sent in advance via the following link:

The osteoarthritis consultation by Markus Klingenberg
The osteoarthritis consultation is a guide for patients with joint degeneration.
“Preserving joints instead of replacing them” is the aim of the experienced orthopaedist and sports physician Dr. Markus Klingenberg. The cartilage doctor provides an entertaining overview of the current state of knowledge on osteoarthritis and its treatment options.
Books on Demand
Where can I order the book and audiobook online?
Also available immediately as an audio book!